|
A Kraft Test is a blood test used to identify a condition known as hyperinsulinemia. It is a picture of how your body responds to food, in particular glucose - the basic component of most of the carbohydrates we eat increasingly in our modern diets. When glucose enters the body it’s important that its concentration in our bloodstream is kept under control, so the body quickly responds to the glucose influx with a regulating hormone called *insulin*. Most of us associate insulin with a treatment for diabetes, and it is. But actually, everybody naturally produces insulin in the pancreas. Some of us need more insulin than others and the particular “pattern” of that response is very telling as to the status of your metabolic health. In fact, many medical professionals think it’s the most important blood test for metabolic health. The reason it is so important is because the test is an early-warning of chronic disease risk. A Kraft Test can reveal if the patient has a condition known as hyperinsulinemia, which is known to increase the risk of a host of conditions including diabetes but also hypertension, heart attack, stroke, neuropathy and even things like tinnitus, vertigo and hearing loss. In fact, Kraft took to calling hyperinsulinemia “occult diabetes” or “hidden diabetes”. In his original study*, Dr. Joseph Kraft, the doctor and pathologist who discovered these patterns, grouped the patterns he observed in patients into five broad groups. These patterns were observed after asking his patients to take a glucose drink while in a fasting state. This allowed him to isolate the behavior of insulin as it responds to glucose over the subsequent 3 hours and is almost exactly the same protocol you will follow to discover your Kraft Pattern. His discoveries were remarkable. He found that of patients who had normal blood glucose levels (about half the population in his study), and who therefore were thought to be in a “normal” or healthy metabolic state, 50% actually had hyperinsulinemia and a further 25% were borderline for the condition. Effectively these people had an early form of diabetes and didn’t even know it. They thought they were fine! The key insight a Kraft Test offers is in the pattern of insulin response to glucose consumption. But what do these patterns actually look like and what do they mean? Let’s take each one in turn. What follows are high-level descriptions and meaning of each Kraft Pattern as described by Crofts*. 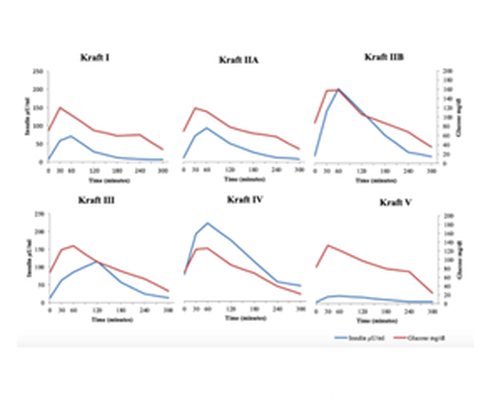 Pattern I
This is the pattern observed in normal metabolically healthy individuals. Note how the insulin responds to the consumption of glucose but does so in a moderate way and rapidly declines after it has done its job. Pattern IIA This pattern is observed in patients who have a “borderline” degree of insulin resistance. Here we see a higher fasting level of insulin (not a good sign) stronger initial insulin (post-glucose drink) concentration in the blood for the simple reason that more of it is needed to keep glucose under control. Pattern IIB This pattern is observed in patients who have what is called hyperinsulinemia - an early biomarker for diabetes risk. Here we once again see a higher fasting level of insulin. Importantly we also see an even stronger initial insulin (post- glucose drink) “spike” in the blood compared to those in Pattern IIA. Pattern III This pattern is also observed in patients who have hyperinsulinemia. Here again we see the characteristic higher fasting an post-glucose-drink insulin levels. But we also see a delayed “tail-off” in insulin as the hormone stays around longer in the blood. This is a more pronounced form of hyperinsulinemia and people with diabetes typically have this kind of pattern. Pattern IV A rarer pattern that some patients will present with. Here we see a very high fasting level of insulin, a non-delayed peak and then a long tail off. Again, this is likely to be a sign of diabetes. Pattern V Pattern V is actually a special case. Note how insulin stays very low throughout the test. This is because these individuals are likely Type 1 Diabetics. The opportunity to get this assessment is now and with new technology you can get a real time assessment at our clinic in Devon. *Detection of Diabetes Mellitus 'In Situ' (Occult Diabetes) - Joseph R. Kraft, M.D. Laboratory Medicine, Volume 6, Issue 2, 1 February 1975, Pages 10–22. Postprandial insulin assay as the earliest biomarker for diagnosing pre- diabetes, type 2 diabetes and increased cardiovascular risk - DiNicolantonio JJ, Bhutani J, OKeefe JH, et al. Open Heart 2017. Identifying hyperinsulinemia in the absence of impaired glucose tolerance: An examination of the Kraft database - Crofts C, Schofield G, Zinn C, Wheldon M, Kraft J. Diabetes Res Clin Pract. 2016 Aug.
0 Comments
A problem with our current diagnosis of metabolic health is our obsession with monitoring glucose and viewing as the metric that matters. In the example below we have the two time points. The first is Insulin Resistance or pre diabetes and important to note the glucose is normal but insulin is elevated they are not the same thing we fail to appreciate that they do not go hand in hand that if glucose is low insulin is low or glucose is high insulin must be high. For an historical point- Dr Joseph Kraft a pathologist developed the kraft test- an Oral glucose tolerance test with insulin assessment. Testing over 15,000 patients he found that in over 50% of confirmed diabetes cases they had normal glucose levels but high insulin. This would have been missed if we only test blood glucose levels. Glucose is obsessively the marker we concentrate on with diabetes but it shouldn’t be! We have the ability to measure insulin, so why don’t we? We see here that insulin is highlighting the problem potentially 10 years before we see a change in blood glucose levels. This is the potential if we come away from a glucose centric paradigm. 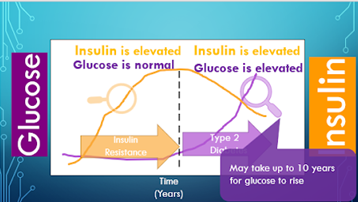 How is hyperinsulinemia caused? 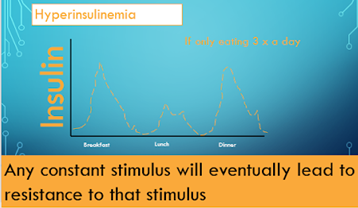 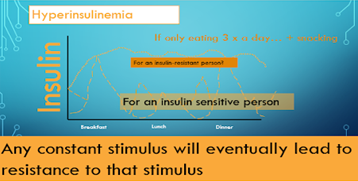 The first eating pattern of 3 meals a day is more of an uncommon eating pattern we see today. Every time you eat this is the reciprocal insulin response across the day. Compare that to the more common pattern of breakfast, mid morning snack, lunch, mid afternoon snack, dinner and possibly dessert. This causes many more insulin responses and with a insulin sensitive person this can be managed for a while. But for an insulin resistant person the insulin never comes down it is constantly elevated. Therefore, we can now see that hyperinsulinemia can be a consequence of insulin resistance and also a cause. Its a vicious cycle accelerating the problem until the person changes their habits. How do we correct insulin resistance? If hyperinsulinemia is the primary cause then lowering insulin needs to be the solution. We do that through the foods we eat and by managing these macro nutrients. Compared to drugs it doesn’t come along with side effects it actually has side benefits to all our metabolic markers and our waistline! How do Macro nutrients affect Insulin? Currently according to the global nutrient database this is the proportion of macro nutrients we are eating around the world, Carbohydrates were the major contributor to energy availability (70·5%), followed by fats (17·4%), and protein (10·5%). Fat does not increase insulin, there is no study that shows that according to Dr Ben Bikman PhD. Protein has a small effect but carbohydrates have a large effect (18). In the image below this is the effect size in a slightly different view. This is not declaring a war on carbs because the type of carbohydrates do matter, but when we acknowledge that hyperinsulinemia is the cause of insulin resistance, one of these diets is going to work much better at removing the offending agent. When we eat these macro nutrients there is a corresponding blood molecule. In diabetes (type 2) which is just a prolonged insulin resistance, which of these nutrients in the blood is the body struggling with. Glucose is the one we obsess over the most and the one we are all eating the most of. “If lifestyle is the culprit, it is also the cure! The food we eat is causing or can cure these metabolic issues! When we look through an insulin lens, we appreciate we just need to lower the insulin by managing our macro nutrients, control carbohydrates, prioritise protein, don’t fear fat, and maybe frequently fast. This can literally cure the problem.” Dr Ben Bikman 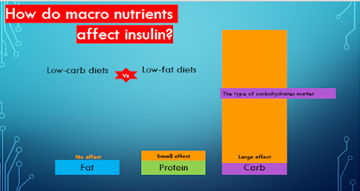 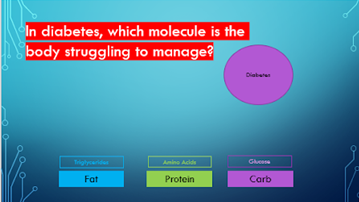 About 5 years ago my health was troubling me as I found it difficult to think
straight, formulate my words, had a lack of energy, motivation for exercise and I was putting on weight. This didn’t make much sense to me as a former athlete and with my job now as a strength and conditioning coach, so I am active all day everyday. I decided to get some blood work done and my triglycerides and HDL were out of the accepted range, which is doubly troubling considering these reference ranges are based on a sick population as it is. This lead me to look for answers and I found those answers and that is what I am going to discuss in this article from my knowledge through my learning through the Nutrition Network which I am now a nutrition Network advisor and the knowledge of many exceptional researchers, clinicians around the globe that have highlighted the impact of insulin resistance on our bodies and brain. Metabolic syndrome has been described as anyone having three of these five symptoms, increased waist circumference, increase in blood glucose, high blood pressure, high triglycerides and low high density lipid proteins or HDL the so called good cholesterol. In the UK currently it is said that 33% of adults have metabolic syndrome (1), this is not just a UK problem this is a global problem with high rates of insulin resistance in south east asia, the middle east, pacific islands, USA and Mexico, which showcases the prevalence of the problem. It is estimated that nearly a billion people suffer from Insulin Resistance across the globe, (2) yet it is not routinely screened. In the UK the problem actually could be a little worse, high blood pressure or hypertension is said to affect 58% of the population (3) which is a critical part of metabolic syndrome and usually the first sign that something has gone array. While we are not always measuring the other signs, we are always measuring blood pressure when we see a GP. So if 58% of the population have hypertension might that mean that 58% have insulin resistance. Why that connection? Metabolic syndrome used to be called Insulin Resistance syndrome which does a much better job at explaining what is causing the symptoms, much better than the vague term metabolic syndrome. So if 58% of people in the UK have hypertension its not much of stretch to suggest they have Insulin Resistance which is presenting itself as high blood pressure. Insulin Resistance is at the root of the common diseases we are seeing today such as Heart Disease, as it is fundamental in contributing to heart Disease and the damage to the vascular system, it would be very uncommon not totally impossible for someone to have heart disease without insulin resistance and hypertension plays into that. With Cancer, some cancers are not caused but made worse by Insulin Resistance, as it accelerates the growth of the cancer cells. Fatty Liver, the most common liver problem across the world, directly caused by insulin resistance and the insulin promoting the growth and the production of fat within the liver. Type 2 diabetes, with the high levels of insulin known as hyperinsulinemia is trying to manage the high blood sugar levels and causing more cells to become resistant, and Body Fat, you cannot make fat cells grow without insulin being elevated, regardless of calories consumed. In addition to these big 5 killers or problems, we have some that range from similarly lethal and tragic like dementia and Alzheimer’s disease, being the most common form and even stroke one of the most top expenses of the NHS. Then less lethal but very relevant to a population and particularly heart breaking for a couple we have the most common forms of infertility. The most common in women PCOS (more appropriately called metabolic infertility) insulin directly affects estrogen production from the ovaries and in Men Erectile Dysfunction which may be the first clinical sign of Insulin Resistance in otherwise healthy men. Due to what IR is doing to the blood vessels. The hope is that a person who is taking medications for hypertension, diabetes, migraine, and fatty liver etc doesn’t believe that they are all individual problems they are in fact the symptoms of the same root cause. Once we know this we can then impact that root cause and as Dr Robert Lustig has suggested in his great book Metabolical, the root cause is not druggable but is foodable. This is because these chronic diseases are disease of the mitochondria the power house of a cell that uses food to produce energy. So while treating the symptoms of these diseases with drugs it never gets to treat the mitochondria, only food can do that. How do you know if you have insulin resistance? Do YOU have high blood pressure, type 2 diabetes or gestational diabetes, PCOS (women), Erectile dysfunction (Men), fatty liver disease, or skin tags and dark patches on the back of the neck or under the arms (acanthosis nigricans). The skin can be a window into the metabolic soul! If you answered yes to anyone of these then you likely have insulin resistance. These are signs of an underlying metabolic problem, but most are undiagnosed! This is why the problem is likely much worse because you could have someone with these skin tags and acanthosis nigricans and have a normal blood sugar or blood pressure and therefore they are not considered to have any issues metabolically. (1)https://www.nhs.uk?conditions/metabolic-syndrome/ (2) PMID: 29480368 (3) https://www.gov.uk/government/publications/health-matters-combating-high-blood- pressure/health-matters-combating-high-blood-pressure Taylormade Performance and rehabilitation teaches Modified Pilates following The Australian Physiotherapy and Pilates Institute (APPI). This method combines traditional Pilates with the most current research into spinal stability. It breaks the exercises down into clearly defined levels to produce a gradual progression of load and control. Using this framework of exercises, we operate in the knowledge that our practices are up to date, safe and effective ensuring the most appropriate outcome for every client. This may be performance related, muscle toning, rehabilitation, posture or just to be able to move more efficiently and free of pain and stiffness. Whatever the objective our program has a proven track record of success.
There are many forms of Pilates from Mat work exercises that utilise the control, resistance and mobility of the body alone to exercises using the reformer, a specific piece of equipment that provides external resistance to exercises. There are various smaller apparatus such as the Pilates Ring, the small over ball, the foam roller, the resistance band and the Barrel to name a few. The modified Pilates method that we practice also provides a host of diversity by creating levels of intensity for each of the original 34 Pilates exercises. The variety and diversity that can be achieved with Pilates makes it such a successful mode of exercising in a group. It allows the instructor to adapt and create a variation of an exercise to cater for different abilities within the same class without setting up completely different programmes for each member of the group. It also provides an opportunity for the participant to witness improvement and progress in their practices. Our tailored approach that underpins all our services is carried through to our Pilates groups. We can achieve this by keeping our Pilates groups small (on average between 4-6 participants), whilst using the modified Pilates approach and the variations it offers. The individual induction we recommend prior to joining a class provides an insight into the participant’s ability, control and experience ensuring they are safely whilst suitably challenged. Pilates is recognised as a beneficial activity for promoting wellbeing. Its exercises focus on a mind and body connection promoting concentration on body awareness and visualisation of movement. It utilises breath work to enhance the performance of exercises. At Taylormade we have experienced further wellbeing benefits expressed by our clients that attend group Pilates. Some groups have practiced together for over six years. This time each week provides opportunity for both new acquaintance and conversation to develop as well as opening up a time for old friends to socialise whilst carrying out their Pilates. Our informal sessions always provide a relaxed and welcoming environment. Pilates is becoming increasingly recognised in the world of sport with top athletes such as Andy Murray, Christiano Ronaldo, Maria Sharapanova, Chris Robshaw and Lebron James all providing testimonies to the discipline.
Pilates can impact an athlete in many ways, 5 key areas are :
What is Pilates:
Pilates is a form of exercise which concentrates on strengthening the body with an emphasis on core strength. Pilates also focuses on the mind-body connection. While doing the various exercises your mind needs to be constantly aware of your breathing and the way your body moves. This form of exercise was developed by Joseph Pilates in Germany where he was a carpenter and gymnast. He invented Pilates as an exercise program for injured dancers and soldiers while living in the UK. Joseph Pilates believed that physical and mental health were closely connected. In the 1920’s he immigrated to the US and opened a Pilates studio in New York. Originally this form of exercise was called Contrology. Today it is widely practiced by many in all aspects of life and its key principles are transferred into our everyday life.
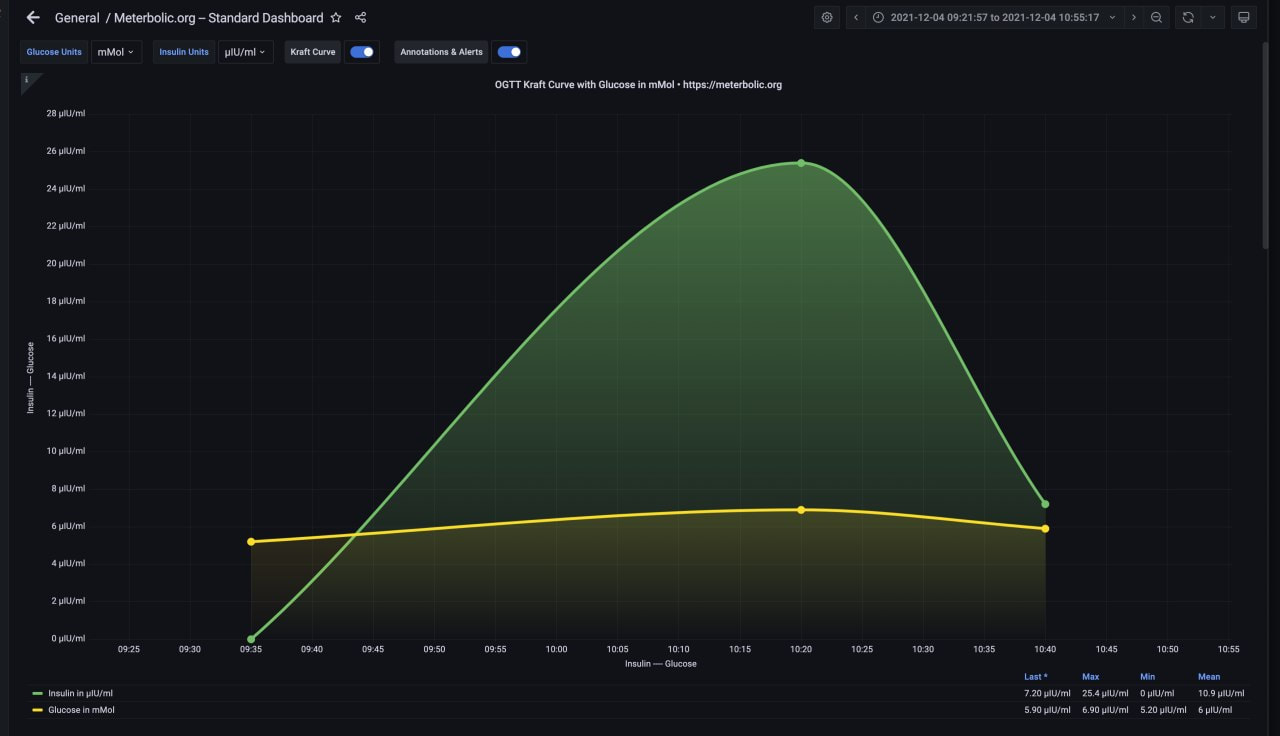
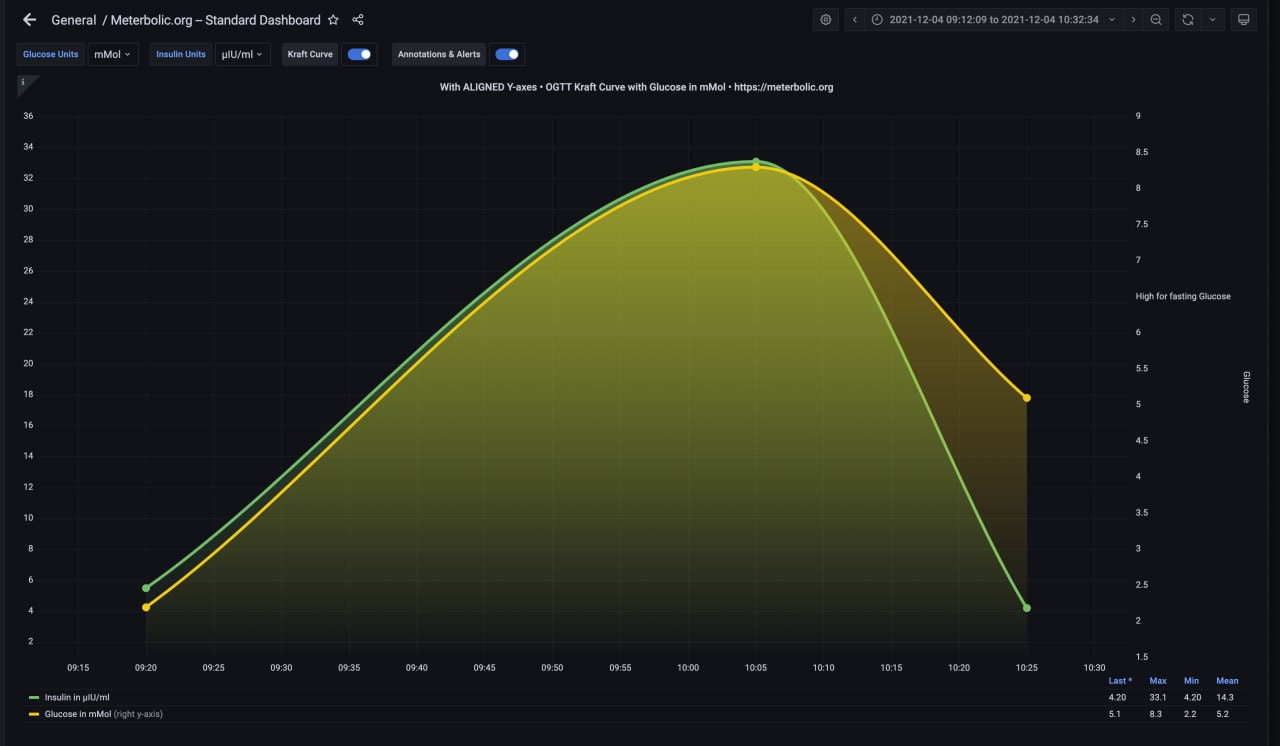
In December we pioneered the first Metabolic Kraft clinic in the UK. Together with Dr Donal Collins and collegue Debbie Cox we tested 7 of my current clients to provide them with real-time Kraft curves and a metabolic profile interpretation like this A “Postprandial insulin assay is the earliest biomarker for diagnosing pre-diabetes, type 2 diabetes and increased cardiovascular risk” Dr James J DiNicolantonio. My clients therefore were eager to know what sort of shape their metabolic health was in. In addition this assessment allows if there is metabolic dysfunction a faster response to lifestyle changes than glucose assessment. Made famous by Dr. Joseph Kraft, a clinical pathologist, who ran 3,650 glucose-insulin tolerance tests. developing what is now known as the Kraft curve. 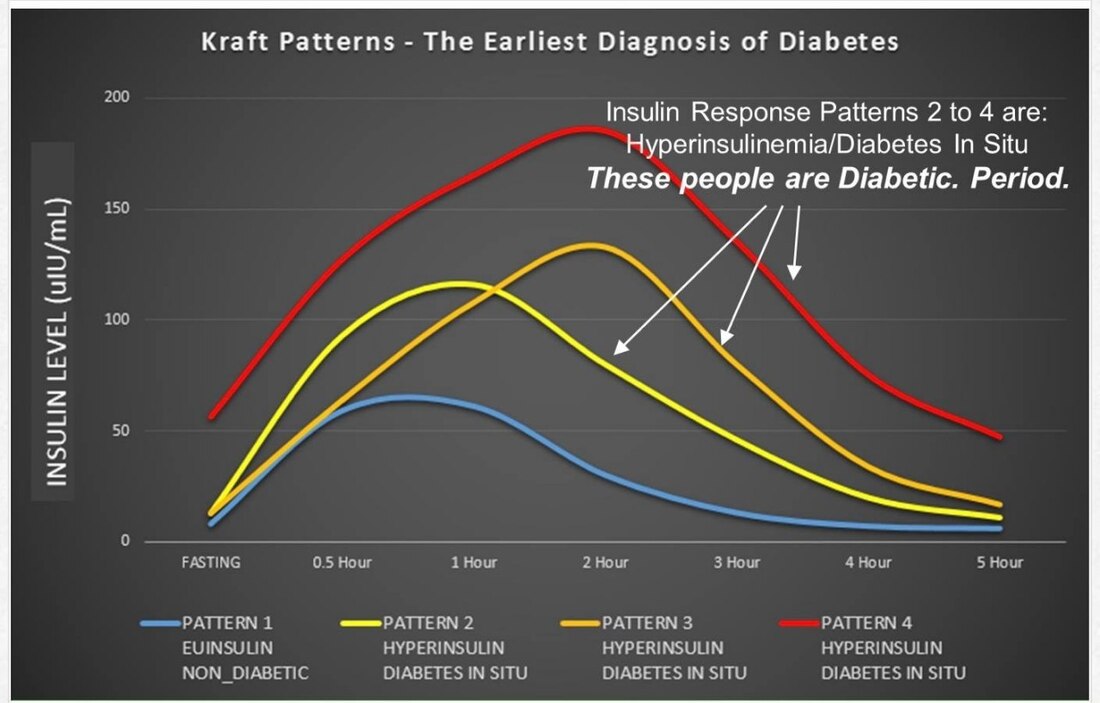 Of the 3,650 glucose tolerance tests, 1,713 were defined as normal (for diabetes mellitus) according to the criteria of the American Diabetes Association.
Of the 1,713 tests which would have been judged normal strictly on the basis of glucose tolerance, 50% were demonstrated abnormal on the basis of insulin tolerance, and another 14% were borderline results. 2.5% were displayed insulin response. This means that 2/3 of the tests that would have been judged normal by the Glucose Tolerant Test were found to be latent diabetic when the Kraft Prediabetes Profile test was taken into consideration. This is the power of insulin assessment! My clients were all in good metabolic health and thoroughly enjoyed the experience and the opportunity to learn more from each other and from themselves in what action they have taken over the last few years is keeping them healthy. Some of the comments from the day were: “It was very enlightening. Pleased my ‘internals’ are working well… must be all the good groundwork we have been putting in” “Thank you for this amazing health check. It is reassuring to know all’s well.” “Great experience, nice to meet other people interested in their health. The whole experience was really well organised and professional. Thank you for the information.” “The new insulin testing offered by Taylormade Performance & Rehab is truly enlightening. Andy’s explanation of insulin’s role in the body and associated potential diseases, coupled with my own personalised insulin resistance profile gave a real insight into my own health. Highly recommend this to anyone who wants to look after themselves both today and for their future selves.” “Long term health has been a key driver for changing my eating habits, I want to be a fit and healthy role model for my children and I want to be around to watch them grow up. The metabolic testing was really part of that whole journey - it confirmed to me that I’m on the right path and that I am healthy- if I hadn’t made the changes I did 2 years ago then based on the results I would most certainly be more at risk of disease and poor long term health.” If you are interested to learn more about the Kraft test pllease also see the soon to be launched site www.meterbolic.org and video attached below. https://youtu.be/SRrT0QT2ALw We would love to add more sites around the UK and the world. So, if this sparks your interest and you want to have a test, support or collaborate, then please drop a DM to myself for information and discussion. Would love to hear from you and discuss your role in the next phase of our Metabolic Revolution! For sports people genetic tests should be the natural base to evaluate how much of their potential they are exploiting.
Many sports people are convinced that adequate training combined with correct nutrition (and here we could open a bible of considerations) permit them to achieve the best performances. However before an allergy there can be an adverse reaction to a food which then becomes an intolerance, but even sooner an adverse reaction is then a reduction in absorption of nutrients, so basically many people have "correct" nutrition that due to different reasons (intestine, genetic predisposition, over feeding) doesn't let them use the 100% of proteins, vitamins etc.etc). On this basis if you accept this concept the first thing to test is the engine, is the "burning efficiency" of the engine working well and checking if the fuel used is the best for that specific engine. So the first easy test to offer is the intolerances one (TIAMI 180 but if the analysed subject is not in particular a food explorer that loves to test and eat anything the TIAMI 90 is more than enough). TIAMI is FOOD INTOLERANCE TEST IMMUNOENZYMATIC METHOD in a Italian TEST INTOLLERANZE ALIMENTARI METODO IMMUNOENZIMATICO (TIAMI). TIAMI 90 crossed with a food weekly journal allows for a clear picture of how much food energy is being exploited in the patient. TIAMI test offers as well the possibility to evaluate intestine wellness 'cause if the patient is eating correct food in terms of tolerance but complains about some problem with intestine (abdominal swelling, difficult or too easy evacuation, acne, excessive sweating, etc.etc) we can presume that there is a dysbiosis in progress that causes an inflammation . What could be worse for our well-being than not doing any kind of physical activity?
Probably do it wrong.... Let’s start from the assumption that we are not all born to do marathons or endurance races like "ironman" then the first consideration that has to be made before venturing into any sport discipline, is what type of exercise best suits us and our actual physical “shape”. With several pounds more than our weight form, when trying to recover our physical fitness to decide to go jogging every evening for 90 minutes is not the most suitable choice, our knees and our back if asked would not agree... We have always to consider that a wellness program starts from a healthy diet developed on our predispositions, our tastes and our lifestyle so, once again, combining homemade or "hungry" food programs with Olympic exercise only leads to stress unnecessarily on our body and our metabolism. We have to be aware that in a slimming program the exercise aspect helps for a 20-30% not anymore. To continue to eat “random” even if combined with the best fat burning exercise does not lead to anything: many people after weeks spent training have not lost weight, and in cases that they have lost it is more in liquids than fat mass. Before starting any sport activity it is always recommended to do a medical examination in order to check our state of health to avoid future problems: if 20 years ago we were a skilled footballer or good tennis player remember that it was 20 years ago. Time unfortunately is not a friend of health and basing our recovery in form in a program on past splendors is not a wise approach. To support well-being 150 minutes per week of aerobic activity are enough; however it’s totally useless to do everything on the weekend and you should try to distribute these 150 minutes on seven days.(20 per day) Often on Sundays you see on the streets "cyclists" who would like to be a Tour de France participant, weighted in pedaling, body and spirit, “veterans” of a 80 miles tour then after that from Monday to Saturday the only sport practiced was the “fridge door opening” convincing themselves that a single exhausting weekly session resolves the "problem" weight/ well-being. It would be enough to look at our profile in the mirror to verify that this is not so. Twenty minutes a day, a little less or more, can be found and it is a small sacrifice that our health will appreciate. If we combine this manageable physical activity with an adequate food plan, based on a preventive medical investigation and not on the diet downloaded from the internet, our silhouette will join the applause of health and we will find ourselves enjoying a new optimal sense of wellbeing. In conclusion: "do it yourself" as it is a cheap choice does not always bring positive results, so we do less but do it better. Don’t work harder work smarter! No drastic and dramatic choices, no low-calorie diets, no exhausting gym session at 9 pm because we don’t have time before: let’s wake up half an hour before, take your breakfast at home, let’s get used to having healthy snacks, eating healthily and taking care of ourselves and our silver years will be better because we have invested a little but consistently. Little but on a regular basis is the best formula that ensures lasting results without stress. Andy Taylor & Dr.Fabrizio Reggiani With 7 in 10 people (in the UK) looking to make health improvements post COVID-19, now is the best time for YOU to make that step.
We use a tailor made approach to your health assessment that looks at your physical, mental, social aspects of your life. Apart from the physical assessment we want you to have an idea on how you feel about yourself and what you are capable of and what areas of your life are a priority for you and what you are putting in place to make those areas as strong as you want them to be. How it works: 1. Measurements •Body Composition Analysis, Body Composition Scales Bioimpedance Analysis (BIA), Tanita, Non-intrusive, Simple print out Takes 20 seconds, •Waist Circumference. Waist to height score •5km Row cardiovascular MAF assessment •Squat, Lunge, Press, Pull, Brace, Hinge Strength Assessment •Wheel of life Assessment, Self Esteem Questionnaire, Self efficacy for exercise Questionnaire 2. Consultation Explain metrics, educate, coach, agree goals & actions before next measure 3. Book follow-up Next appointment in 3 month period Membership provides x4 measures per year for £240 Monthly Assessment £720 per year THIS IS NOT A GYM MEMBERSHIP. This is a Health Membership. However….. We do offer a Supplementary Scheme which includes •Online training remote or via app; 1-1 or Group Workouts, Classes, etc. •Coaching, Remote coaching, Personal training, Pilates etc. •Nutrition coaching, advice, food delivery, meal preparation •Education Seminars •DNA Testing, blood testing ...and much more We are pleased to be offering our clients and you the opportunity to use the Pulseroll products and purchase them through our website.
We have been using the products with our clients over the last two months and the feedback has been so good that we have jumped at the chance to be able to offer our clients and you the opportunity to purchase their scientifically proven products with unique features. The Pulseroll Vibrating Foam Roller PRO with its wider length than the classic roller, the Pro is the most powerful product in the Pulseroll family. Due to the vibrations, there is almost NO need to roll, technique is minimal and it is far less painful to use than a traditional foam roller. Reduce Next Day Soreness and Muscle Pain, 5 speed variations, Controlled easily with the one-touch remote control Percussion Mighty Mini Massage Gun The mini massage gun has been designed to be your pocket-friendly ally. It helps to keep aches and pains at bay wherever and whenever they occur. Reduce Next Day Soreness and Muscle Pain, Increase Blood Flow and Flush Away Lactic Acid, Perfect to use all over the body. Pulseroll Percussion Massage Gun PROThe Pulseroll Massage Gun PRO treats problem areas with short, strong pulses. A hand-held deep-tissue tool that uses rapid strokes to stimulate blood flow to the muscles. Reduce Next Day Soreness and Muscle Pain, Increase Blood Flow and Flush Away Lactic Acid, Perfect to use all over the body Pulseroll Vibrating Massage Peanut BallThe innovative peanut shape ideally fits comfortably around the muscles, targeting the desired area with precision and best suited for myofascial release, trigger point therapy, and deep tissue massage. Can be used on almost any part of the body, Controlled easily with the one-touch remote control, Portable and Lightweight Pulseroll Vibrating Massage Single BallSmall but powerful; the Pulseroll Single Ball helps to reach and specifically target trigger points, combined with our vibration technology that can penetrate deeper into the desired muscle fibres. 4 vibration settings, Can be used on almost any part of the body, Portable and Lightweight. All products have been scientifically proven Scientifically Proven to Reduce Next Day Soreness and Muscle Pain, Increase Blood Flow and Oxygen to Muscles and have been Approved by Physio's and Pro Athletes. To get hold of the product you need today check out our online shop to order https://www.taylormaderehab.com/store/c10/Sleep_and_Health.html#/ At Taylormade we are acutely aware of the demands of juggling a business or businesses with family life. We understand that to be truly productive in every area of your life requires a concerted effort to manage your time and to make sure that time is well spent in the support to your wellbeing and your productivity.
Therefore, we have created a programme that maximises the time you spend in developing your health, strength & happiness. Our 30minute programme with sessions on a Monday & Thursday morning with classes between 6.30-7 & 7.15-7.45am is ideally placed to optimise the start to your day. Ground in neuroscience being up early in the day giving you the opportunity to get morning light on your eyes that increases alertness and is the most important strategy you can do to support your mental and physical health (metabolic wellbeing, positive function of your hormone system, mental health steering in the right direction). This means getting outside even if there is cloud cover without sunglasses, how long depends on the brightness of the morning from 5mins-30 mins (minimum to fantastic). The neurons that pick this light up convey to the brain that it is daytime and time to be alert. Ok so back to the exercise once you have your alertness. How does exercise impact your brain and health? Data going back to the 1990s supports the idea that physical movement of particular kinds can support brain health and brain function both in the immediate term and long term. So it should have a profound impact on how you structure your day. Getting blood flow to the brain; The brain is an organ too, it is the most metabolically demanding organ in your body, its receiving those metabolic factors, those fuels by way of the vasculature blood vessels, capillaries and veins and things of that sort. So movement is very crucial to get your brain to function properly and movement of various kinds actually. Resistance training turns out to be as important as endurance training because of the way it stimulates the release of particular hormones actually from bones, things like osteocalcin, which can positively impact brain function and support the health of existing neurons as opposed to increasing the number of neurons (increasing the number of neurons turns out may not be as beneficial as we may think due to incorporating new neurons into existing circuitry is actually very challenging for the brain to do). So why 30 mins? Working out for too long- over an hour can be detrimental because of raising cortisol which is not always bad if it is appropriately timed and the appropriate low levels but you don’t want your cortisol levels up through out the day or big spikes in cortisol repeatedly, so keeping workout bouts relatively short can help with that so shorter bouts of exercise is more optimal. So getting the timing and exercise combination right across your week, not too long or too short has been shown to be immensely beneficial for things like brain derived neurotrophic factor (increased connections in the brain), limiting inflammatory cytokines, for promoting anti-inflammatory cytokines, provided the exercise is of the proper duration and that its not so intense that your actually creating damage to the various systems of the body and your health breaks down. Strength training with Taylormade is about stimulus to fatigue ratio to get optimal muscle hypertrophy. The optimal stimulus to grow more muscle. Crossfit for example = tons of fatigue but you never really hit failure super deliberately in any muscle group so the stimulus to fatigue ratio is horrible. So in our programme the goal is the highest stimulus to fatigue and the lowest time and equipment and remember the reasons for not thrashing yourself for long periods of time with lots of fatigue is that this can be detrimental to your health and we want to optimise your health so you can start to see how it fits the literature and research. With the protocol we use you get greater stimulus for hardly any fatigue and hardly any time constraints with hardly any equipment which means that outside of our coached sessions you can continue at home. By trading intensity for duration, we can get our health benefits in a time frame that fits into your daily life. The highest lean mass to the lowest fat mass with this type of training and our nutrition advice also will help to maintain your metabolic health which means that the risk of diabetes, stroke, cardiac failure are all massively reduced. If you are someone with limited time and your health is a priority then please send us an enquiry to learn more and to find out about the other parts of our programmes from nutrition, programming, pilates, injury management and mindfullness training to incorporate on your health journey. https://www.taylormaderehab.com/general-enquiry.html#/ Physical activity and health have never been more important than they are right now. We all know the physical and mental benefits of exercise but with the addition of the COVID-19 pandemic it has brought peoples health into the spotlight. It has been reported that people less physically active prior to getting COVID-19 have a higher risk of severe outcomes from the virus than those who are regularly physically active, according to a new study “Physical inactivity is associated with a higher risk for severe COVID-19 outcomes:a study in 48,440 adult patients, published in the British Journal of Medicine, April 13th.”
As we try to immunise the world, the most likely scenario for the next few years is that COVID-19 will be more like other infectious diseases, such as flu, that we will continuously manage and protect ourselves against. Exercise is one of the best ways to do that. We know that physical activity is one of the most effective ways to prevent chronic diseases, along with diet and quitting smoking. A study in 2008 found that physical inactivity is responsible for more than five million premature deaths every year- “Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy, The Lancet, 2012.” It is important that anyone taking part in a new exercise regime understands their current health status and that the regime meets the individuals current ability level, so that additional stress is not put on the body. It is also helpful if the development of physical activity and movement quality can be achieved gradually over time and there is an assessment whereby the individual can see progress . Anyone returning to exercise after contracting Covid 19 should be aware of the current Considerations and recommendations for recreational athletes returning to activity after COVID-19. "Considerations- Each patient with COVID-19 is unique. Although general patterns in COVID-19 have been reported, there is a wide variance of disease expression. Each patient with COVID-19 recovers at a unique rate. There is currently no algorithm guiding a patient’s stepwise return to activity. The severity of disease appears to affect the duration of recovery, although this has yet to be proven. Return to activity after COVID-19 should be guided by a body-system approach that includes the cardiac, pulmonary, hematologic, musculoskeletal, and gastrointestinal systems. Clinicians should advise patients to return to activity in a slow, gradual, stepwise manner. Patients should be given instructions to speak with their health care provider should they develop symptoms in the body systems listed above. Recommendations- Exercise should not resume if a patient with COVID-19 has persistent fever, dyspnea at rest, cough, chest pain, or palpitations. Any COVID-19 patient with an underlying cardiovascular or pulmonary condition should consult a physician prior to resumption of exercise, even if asymptomatic. An otherwise healthy patient with a self-limited course of COVID-19 who has been asymptomatic for 7 days may begin resuming physical activity at 50% of normal intensity and volume. Consultation with a physician is recommended if patients who have had COVID-19 develop chest pain, fever, palpitations, or dyspnea on the resumption of exercise." https://link.springer.com/content/pdf/10.1007/s11420-020-09777-1.pdf Jordan D. Metzl, MD & Kathryn McElheny, MD & James N. Robinson, MD & Daphne A. Scott, MD & Karen M. Sutton, MD & Brett G. Toresdahl, MD. Considerations for Return to Exercise Following Mild-to-Moderate COVID-19 in the Recreational Athlete. HSSJ (2020) 16 (Suppl 1):S102–S107 To see the range of services that we provide, that can help you achieve a greater degree of health and wellbeing please go to our services page or contact us page so we can answer any of your queries. https://www.taylormaderehab.com/services.html#/ https://www.taylormaderehab.com/contact.html#/  The human body has to be considered like a soil.
When we are young our body is rich in nutrients: minerals, vitamins, and hormones combined with a healthy and balanced diet to help keep this perfect "world" in balance. Life, however, hardly offers to us optimal epigenetic conditions that permit to maintain these conditions over time: frenetic rhythms, stress, little exercise, bad diet, medicines in addition to natural ageing lead us from the age of 35 years on wards to impoverish this soil. Through the years, the blood tests clearly show that mineralogical and vitamin deficiencies are more and more frequent with the consequent increased possibility to favor the onset of different pathologies. To maintain these values optimally, unfortunately, the diet even if healthy, is not enough, because it also depends on a number of factors related to the environment in which we live, the work we do and, in women, pregnancies, menopause and other factors mean we need help. Nutriceutical science based on natural organic phytotherapy products helps to restore and maintain optimal levels of nutrients, helping also to modulate the hormone levels related to the proper functioning of organs essential to optimal metabolism. Why organic? Our body is not a sponge that absorbs any substance. Supplements of chemical and synthetic origin are marginally absorbed by our organs in the indicative measure of 10% while products of organic origin are absorbed around at 90%. And this must be a clear evaluation parameter for those who need supplements. However it should be underlined that dietary supplementation should be made exclusively under medical supervision and not following self-proclaimed advertisements that promise miraculous results by taking supplements or multivitamins often of chemical origin or under the advice of people who do not have a specific medical preparation; even worst when we rely on word-of-mouth. What was good, assuming that what really brought positive results and always carefully considering the placebo effect triggered by expectations rather than real effects, to our best friend does not mean that it will be good for us too. Taking supplements without knowing what our corresponding physiological levels are, related to elements we are taking, at best it wastes money because with already optimal levels we will dispose through urine and feces the "miraculous" effect, and then how useless a supplement will be. Often, however, an uncontrolled and probably useless intake involves fatigue for kidneys and liver, intestinal inflammation risking to cause disorders or trigger latent pathologies such as allergies, intestinal intoxication and dysbiosis as well as being able to present possible allergic interactions with any current drug treatments. It is therefore necessary to pay attention to what we take in the form of a supplement because there is no seasonality, age or climatic conditions that require universal intake of food supplements, but an individual physiological need that must be previously verified and evaluated by a medical professional in the sector. Through specific blood tests we can establish what your body really needs for your wellness in a dedicated program that will take care of your diet, fitness and any need of your body to achieve the best well being. Contact us for a no obligation consultation to find out how the support of supplements can aid any vitamin deficiencies you may have in the most natural way possible. Dr Fabrizio Reggiani and Andy Taylor  The fact that the intestine is our second brain is no longer a new concept.
The enteric nervous system of the digestive system contains 500 million neurons and represents a real autonomous system that affects the central nervous system (brain and marrow). Many people suffer from depression, hypersensitivity, intestinal dysbiosis, intestinal irregularities, being overweight, which are all factors that affect our well-being. Although several of the listed disorders are sometimes associated with neurological processes, the central nervous system is not always the only one responsible as it interacts with the whole physiological system of the person. - Difficulty in sleeping - Difficulties in concentration - Increase, loss (rarely) or difficulty in weight control - Hyperactivity or motor retardation - Moody or depressed These are the typical symptoms of an intestine that does not work optimally. These alterations are often associated with deficiencies in the gut microbiota (the set of micro-organisms found in our intestines), which carries out and contributes to numerous physiological activities; from synthesising nutrients and vitamins, to helping the digestion of the food we ingest, to modulating the levels of hormones, cortisol, and adrenaline, which when high contribute to stress. The Immune system, which is of the greatest importance through the Covid-19 epidemic especially, is found in the intestine. A nonperforming intestine is a facilitator of diseases! Various diagnostic solutions have been developed on these scientific considerations and patient needs: microbiota and intestinal permeability tests carried out on patients suffering of depression, stress and overweight revealed serious deficiencies and alterations affecting mood, basal metabolism, immune system, neuroendocrine and the neural system. Intestinal tests are not invasive, just a self blood sample with a finger prick and a urine sample to be able to have a complete overview of health conditions of our intestines and are therefore suitable for every type of patient of any age. The rehabilitative treatment is often "simply" based on the assumption of prebiotics and probiotics, not medicines, that combined with a food rehabilitation program and moderate exercise allow you to regain intestinal well-being, the physical form but also the serenity of the gut. We offer several personalised tests on the microbiota and intolerance's that have already solved dozens of cases of patients "apparently" suffering of "pathologies" that instead were attributable to a low-performing intestine and an altered microbiota. Once the intestine has been fixed, the other disorders have disappeared or fallen to manageable levels with proper nutrition and simple natural remedies, regulating and optimising the metabolism of the person allowing him\her to control their weight more easily. This topic would certainly deserve more space and insight that our consultants will be happy to provide you during an informative interview without commitment focused on your needs. Dr.Fabrizio Reggiani & Andy Taylor here to edit. |
Taylormade
|

 RSS Feed
RSS Feed
|
|
PERFORMANCE AND REHABILITATION CLINIC
Injury Management and Conditioning Specialist
Taylormade Rehab, 1 Belle Vue, Fenny Bridges, Honiton, Devon EX14 3BJ | 07800 824557 | 07855 386634
© 2019 Taylormade | Performance & Rehabilitation Clinic. Injury Management & Conditioning Specialists | Website design by brightblueC
© 2019 Taylormade | Performance & Rehabilitation Clinic. Injury Management & Conditioning Specialists | Website design by brightblueC